Knee
The knee is a critical component of the lower extremity and is often subject to injury and a common site of pain in children and adolescents.
Common knee conditions, procedures and injuries affecting children and adolescents:
- Knee Pain in Children and Adolescents
- Range of Motion and Stretching Exercises
- Discoid Meniscus
- OSGOOD-SCHLATTER DISEASE
(Osteochondrosis, Apophysitis of the Tibial Tubercle) - Anterior Cruciate Ligament
- Osteochondritis Dissecans
- Knee Arthroscopy
- Plica Syndrome
Knee Pain in Children & Adolescents
Description
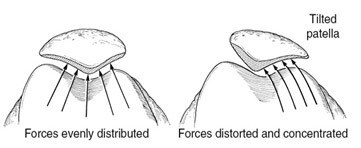
Parapatellar knee pain, sometimes referred to as Chondromalacia patella is characterized by pain in the knee due to increased pressure from the kneecap (patella). This usually occurs without injury, although it may follow injury to the knee. The patella is a V-shaped bone that sits in a groove (trochlea) of the thigh bone. The kneecap is a bone within the tendon of the quadriceps muscles (thigh). The patella stays within the groove in the thigh bone because of muscle forces and ligament-like tissue (retinaculum).
Common Signs and Symptoms
- Diffuse knee pain, usually in the front half of the knee, behind the kneecap, or in the very back of the knee; pain may also be above or below the kneecap
- Pain that worsens with sitting for long periods, arising from a sitting position, going up or down stairs or hills, kneeling, squatting, or wearing shoes with heels
- Often, pain with jumping
- Usually achy pain but may be sharp
- Giving way, catching of the knee
- Minimal or no swelling, no locking
Causes
This condition usually occurs without injury, although it may follow an injury to the knee. Weakness of the quadriceps muscles (which follows knee swelling or injury) results in poor tracking of the kneecap. Poor tracking also occurs in individuals with poor alignment of the whole thigh and leg. The poor tracking results in pressure being concentrated on the outer part of the kneecap (as opposed to being distributed over the whole kneecap). The retinaculum on the inner part of the knee is stretched while the retinaculum on the outer part of the knee shortens with time. The pain is worse when the knee is bent or when the quadriceps muscle is active or both (each causing force on the patella).
General Treatment Considerations
Initial treatment consists of medications and ice to relieve pain and reduce inflammation, stretching and strengthening exercises, and modification of the activity that produces the symptoms. These may be carried out at home, although occasionally referral to a physical therapist or athletic trainer may be indicated. Icing the knee after exercise is helpful. Occasionally your physician may recommend bracing with a knee sleeve to help the kneecap track properly. Arch supports (orthotics) are helpful for those with flat feet. Surgery may be required if symptoms persist despite conservative treatment. This may be done with or without the use of arthroscopy, by cutting the retinaculum on the outer side of the knee (lateral release) with or without tightening the retinaculum on the inner side of the knee. Occasionally surgery to cut the tibial tubercle (insertion of the patellar tendon into bone) and move it may be required.
Medication
- Nonsteroidal anti-inflammatory medications, such as aspirin, Motrin (ibuprofen) ________________or Alleve (naproxen sodium) ____________________ (do not take within 7 days before surgery), or other minor pain relievers, such as acetamino-phen, are recommended. Take these as directed by your physician. Contact your physician immediately if any bleeding, stomach upset, or signs of an allergic reaction occur.
- Stronger pain relievers may be prescribed as necessary by your physician, usually only after surgery. Use only as directed and only as much as you need.
- Injections of corticosteroids may uncommonly be given to reduce inflammation.
Risk Increases With
- Tight hamstring (back of the thigh), quadriceps (front of thigh), or calf muscles; weak quadriceps (front of the thigh) muscles
- Inadequate warm-up before practice or competition
- Sports that involve running, jumping, or squatting
- Poor alignment of the legs (knock knees, kneecaps that point toward each other when the feet are straight ahead), poorly formed trochlea (something you are born with), flat feet
- Previous injury or surgery to the knee
- Direct injury to the kneecap (falling on the kneecap)
Preventive Measures
- Appropriately warm up and stretch before practice and competition
- Maintain appropriate conditioning:
- Thigh, knee, and calf flexibility
- Muscle strength and endurance
- Use arch supports (orthotics), knee pads
Expected Outcome
Usually curable with appropriate treatment. Complete healing is quickest with rest from offending activity, although continued sports and aggravating activity does not usually lead to irreversible problems or damage.
Possible Complications
- Frequent recurrence of symptoms and disability severe enough to diminish an athlete’s competitive ability
- Arthritis of the kneecap
- Kneecap dislocations
- Risks of surgery, including infection, bleeding, injury to nerves (numbness, weakness, paralysis), knee stiffness, dislocation of the kneecap, weakness, continued pain, compartment syndrome (when surgery is performed to cut the bone of the leg and move it)
Heat and Cold
- Cold is used to relieve pain and reduce inflammation for acute and chronic cases. Cold should be applied for 10 to 15 minutes every 2 to 3 hours for inflammation and pain and immediately after any activity that aggravates your symptoms. Use ice packs or an ice massage.
- Use heat before performing stretching and strengthening activities prescribed by your physician or physical therapist. Use a heat pack or a warm soak.
Notify Our Office If
- Symptoms get worse or do not improve in 6 to 8 weeks despite treatment
- Any of the following occur after surgery:
- Pain, numbness, coldness, or discoloration (blue, gray, or dusky) in the foot
- Fever, increased pain, swelling, redness, drainage, or bleeding in the surgical area
- New, unexplained symptoms develop (drugs used in treatment may produce side effects)
From Scuderi GR, McCann PD, Bruno PJ: Sports Medicine: Principles of Primary Care. St. Louis, Mosby, 1997, p. 368.
Range of Motion and Stretching Exercises
Excessive Lateral Patellar Compression Syndrome These are some of the initial exercises you may start your rehabilitation program with until you see your physician, physical therapist, or athletic trainer again or until your symptoms are resolved. If any of these exercises causes pain or discomfort stop them and consult your physician, physical therapist, or athletic trainer. Please remember:
- Flexible tissue is more tolerant of the stresses placed on it during activities
- Each stretch should be held for 20 to 30 seconds
A gentle stretching sensation should be felt.
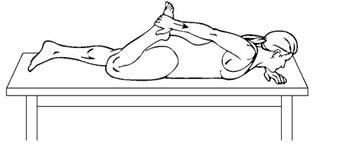
STRETCH - Quadriceps, Prone
- Lie on your stomach as shown.
- Bend your knee, grasping your toes, foot, or ankle. If you are too “tight” to do this, loop a belt or towel around your ankle and grasp that
- Pull your heel toward your buttock until you feel a stretching sensation in the front of your thigh
- Keep your knees together
- Hold this position for 30 seconds
- Repeat exercise 2 times, 2 times per day
FLEXIBILITY - Hamstrings, Doorway
- Lie on your back near the edge of a doorway as shown
- Place the leg your are stretching up the wall keeping your knee straight
- Your buttock should be as close to the wall as possible and the other leg should be kept flat on the floor
- You should feel a stretch in the back of your thigh
- Hold this position for 30 seconds

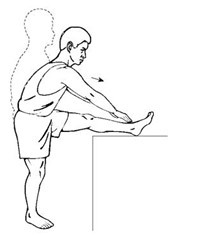
STRETCH - Hamstrings, Ballet
- Stand and prop the leg you are stretching on a chair, table, or other stable object
- Place both hands on the outside of the leg you are stretching
- Make sure that your hips/pelvis are also facing the leg you are stretching
- Slide your hands down the outside of your leg
- Lead with your chest/breast bone. Keep your chest upright and back straight. Do not hunch over at the shoulders. Keep your toes pointing up
- You should feel a stretch in the back of your thigh
- Hold this position for 30 seconds
- Repeat exercise 2 times, 2 times per day
Strengthening Exercises
Excessive Lateral Patellar Compression Syndrome These are some of the initial exercises you may start your rehabilitation program with until you see your physician, physical therapist, or athletic trainer again or until your symptoms are resolved. Please remember:
- Strong muscles with good endurance tolerate stress better.
- Do the exercises as initially prescribed by your physician, physical therapist, or athletic trainer. Progress slowly with each exercise, gradually increasing the number of repetitions and weight used under their guidance.
Only do your exercises in a pain-free range of motion. If the exercises that involve bending your knees while bearing weight cause pain, stop them and consult your physician, physical therapist, or athletic trainer.
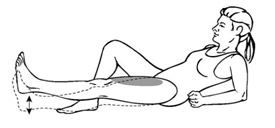
STRENGTH - Quadriceps, Short Arcs
- Lie flat or sit with your leg straight
- Place a _____ inch roll under your knee, allowing it to bend
- Tighten the muscle in the front of your knee as much as you can, and lift your heel off the floor
- Hold this position for 30 seconds
- Repeat exercise 2 times, 2 times per day
Additional Weights: OK TO USE DO NOT USE!!!
If okay’d by your physician, physical therapist, or athletic trainer, a _____ pound weight may be placed around your ankle for additional weight.

STRENGTH - Quadriceps, 7 Count
The quality of the muscle contraction in this exercise is what counts the most, not just the ability to lift your leg!
- Tighten the muscle in front of your thigh as much as you can, pushing the back of your knee flat against the floor
- Tighten this muscle harder
- Lift your leg/heel 4 to 6 inches off the floor
- Tighten this muscle harder again
- Lower your leg/heel back to the floor. Keep the muscle in front of your thigh as tight as possible
- Tighten this muscle harder again
- Relax
- Repeat exercise 3 times, 2 times per day
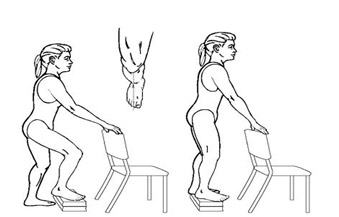
STRENGTH - Quadriceps, Step-Ups
- Use a step or books
- Place your foot on the step or books approximately 6 inches in height. Make sure that your kneecap is in line with the tip of your shoe or your second toe
- Hold on to a hand rail, chair, wall, or another object for balance if needed
- Slowly step up and down. Make sure that the kneecap is always in line with the tip of your shoe or your second toe. Lightly touch the heel of the opposite leg to the floor and return to the starting position
- Repeat exercise 10 times, 3 times per day
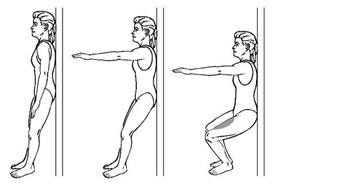
STRENGTH - Quadriceps, Wall Slide
- Stand with your back against the wall. Your feet should be shoulder-width apart and approximately 18 to 24 inches away from the wall. Your kneecaps should be in line with the tip of your shoes or your second toe.
- Slowly slide down the wall so that there is a _____ degree bend in your knees. (Your physician, physical therapist, or athletic trainer will instruct you how to progress the amount of bend based on your symptoms and diagnosis.)
- Hold this position for 30 seconds. Stand up and rest for 30 seconds
- Repeat exercise 3 times, 3 times per day
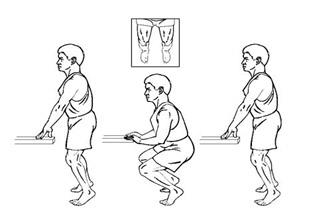
STRENGTH - Quads
- Stand with your feet shoulder-width apart and place equal weight on both legs
- Keep your kneecaps in line with your toes
- Slowly bend both knees, keeping equal weight on both legs, and return to a standing position
- Do not bend your knees more than 90 degrees
- You may use the edge of a table or counter for balance if needed
- Repeat exercise 3 times, 3 times per day
STRENGTH - Quads
- Stand on the edge of a step/stair. Make sure your kneecap is in line with your second toe
- Slowly step down and touch the heel of your opposite leg on the stair below you. Return to the starting position
- Do not go into a painful range. Stop short of the step if necessary to avoid any pain
- Use your stair rails for balance as needed
- Repeat exercise 3 times, 3 times per day

Anterior Cruciate Ligament Injuries
One of the most common knee injuries is an anterior cruciate ligament sprain or tear.
Athletes who participate in high demand sports like soccer, football, and basketball are more likely to injure their anterior cruciate ligaments.
If you have injured your anterior cruciate ligament, you may require surgery to regain full function of your knee. This will depend on several factors, such as the severity of your injury and your activity level.
Click here to know more about to Anterior Cruciate Ligament Injuries.
Knee Arthroscopy
Arthroscopy is a common surgical procedure in which a joint (arthro-) is viewed (-scopy) using a small camera. Arthroscopy gives doctors a clear view of the inside of the knee. This helps them diagnose and treat knee problems.
Technical advances have led to high definition monitors and high resolution cameras. These and other improvements have made arthroscopy a very effective tool for treating knee problems. According to the American Orthopaedic Society for Sports Medicine, more than 4 million knee arthroscopies are performed worldwide each year.
Description
Arthroscopy is done through small incisions. During the procedure, your orthopaedic surgeon inserts the arthroscope (a small camera instrument about the size of a pencil) into your knee joint. The arthroscope sends the image to a television monitor. On the monitor, your surgeon can see the structures of the knee in great detail.
Your surgeon can use arthroscopy to feel, repair or remove damaged tissue. To do this, small surgical instruments are inserted through other incisions around your knee.
Click here to know more about to Knee Arthroscopy.
You will need the Adobe Reader to view and print the above documents. 