Hip
Developmental Dislocation/Dysplasia of the Hip (0-18 months of age)
Introduction:
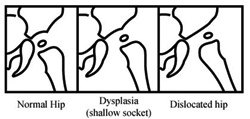
In DDH (developmental dysplasia of the hip) the ball of the hip joint is either partially or completely dislocated out of the socket. Prompt recognition and treatment in the newborn period provides the best chance for subsequent normal hip development. The hip must be perfectly normal to last a lifetime.
Examination:
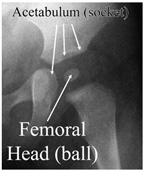
The hip joint is a ball and socket joint consisting of the femoral head (ball) and the acetabulum (socket). With dislocation of the hip, the femoral head is completely out of the socket. In hip dysplasia, the acetabulum has not formed adequately to make a deep socket for the femoral head. Generally neither of these conditions cause a child to have hip pain, however it is necessary to correct the condition early in life to prevent pain as a teenager (early arthritis), and the possible need for hip replacement surgery later in life.
Examination:
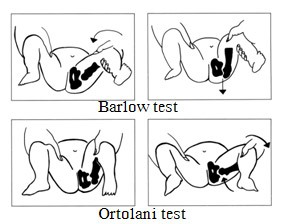
The Barlow and Ortolani tests are clinical exams that evaluate hip stability in infancy. These gentle maneuvers will not harm a child, even if the child does not have hip dysplasia.
Hip Imaging:
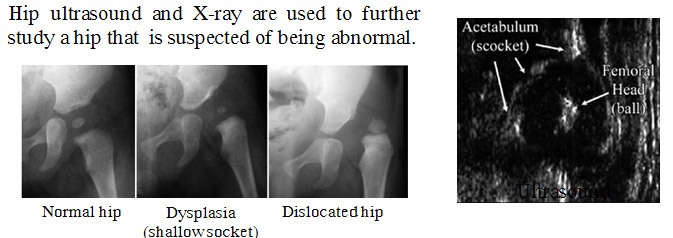
Hip ultrasound and X-ray are used to further study a hip that is suspected of being abnormal.
Treatment:
In a newborn infant with an unstable hip, a short treatment course usually corrects the problem. In a completely dislocated hip, treatment is more prolonged. Holding the infants thighs and legs apart centers the ball into the socket and allows for gradual deepening of the socket (acetabulum). This can be accomplished with the Pavlik harness (in use for more than 50 years).
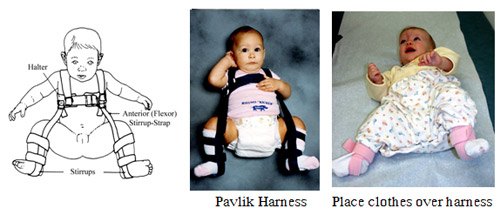
Pavlik Harness:
The Pavlik harness can be used in infants with limited hip motion (abduction) and ultrasound or X-ray abnormalities. The Pavlik harness is generally used for 2-3 months for 23 hours a day and may be followed by a short period of nap and nighttime wear.
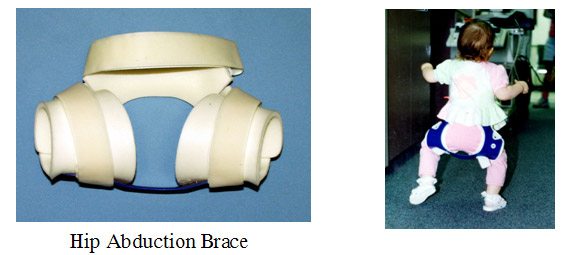
Hip Abduction Brace:
In some cases the Pavlik harness is followed by a hip abduction brace. In cases diagnosed after age 6 months the abduction brace is sometimes used as a primary form of treatment (for mild dysplasia). The hip abduction brace is worn full or part time (depending on the degree of dysplasia). This brace allows a child to walk (cruise). None of these braces will slow your child’s developmental milestones.
Summary:
Hip dysplasia is an important childhood condition and once diagnosed, requires rigorous treatment to avoid premature hip arthritis. Although parents may be upset that their child has to wear a harness or brace, it is important to know that this method is used to avoid more vigorous treatment methods (body cast, surgery) which are required in difficult cases where non-operative methods fail. With proper parental understanding and cooperation most children with hip dysplasia can be successfully treated without casts or surgery.
Developmental Dislocation/Dysplasia of the Hip (> 18 months of age)
Developmental dysplasia of the hip (DDH) or Hip dysplasia is a condition which is seen in infants and young children as a result of developmental problems in the hip joint. The femur (thigh bone) partially or completely slips out of the hip socket causing dislocation at the hip joint. It is most common in first born baby with family history of the disorder. The exact cause for hip dysplasia is not known. Genetic factors play an important role in causing this birth defect. DDH can be mild or severe and can affect one or both hips. It is more common in girls and usually affects the left hip. DDH does not cause any pain and so the condition may not be noticed until the child starts to walk.
The common symptoms of hip dysplasia include:
- Position of the legs may differ (dislocated hip may cause leg on that side to turn outwards)
- Restricted movement on the side of hip dislocation
- The leg may appear shorter on the side where hip is dislocated
- Skin folds of fat on the thigh or buttocks may appear uneven
In normal hip, the head of the femur (thigh bone) fits well into the socket (acetabulum) whereas in hip dysplasia, the socket and femoral head are not congruent because of their abnormal development. During hip examination, the doctor may also look for the difference in range of motion of the hip, presence of uneven skin folds around the thigh and difference in leg length from side to side. In infants less than 6 months, an ultrasound may be advised to confirm the diagnosis.
The treatment for DDH depends on both the age of the child and severity of the condition. The aim of treatment is to keep the femoral head in good contact with the acetabulum so that the hip can develop normally. A pavlik harness may be used to keep the hip in flexion and abduction may be advised. Only when conventional treatment is not effective, surgery to put the hip back into place may be advised.
Residual Acetabular Dyplasia
Coming soon
Legg-Calve-Perthes Disease
Legg-Calve-Perthes Disease (LCPD) or Perthes disease is a disorder of the hip that affects children, usually between the ages of 4 and 10. It usually involves one hip, although it can occur on both sides in some children. It occurs more commonly in boys than girls.
The cause of Legg-Calve-Perthes Disease is not clearly known. It may occur due to inadequate blood supply to the ball of the hip joint (the femoral head) which leads to death of the bone. Over the course of several months, the blood supply returns back to the bone tissue and new bone cells gradually replace the dead bone over 2 - 3 years.
Some signs and symptoms of Perthes disease include:
- Walking with a limp (painless limp)
- Pain or stiffness in the hip, groin, thigh or knee
- Shortening of leg or unequal leg length
- Wasting of thigh muscles
Your doctor will make a diagnosis based on your child’s signs and symptoms, a thorough physical examination, imaging studies such as X-ray of the hip, and magnetic resonance imaging (MRI) scan.
Treatment
The goal of treatment for Perthes disease is to keep the femoral head snug in the socket portion of the joint. Nonsurgical treatment options may include rest, activity restrictions, anti-inflammatory medications, casting or bracing, and physical therapy. If nonsurgical treatments don't work, your child may need surgery. Surgery involves lengthening a groin muscle or reshaping the pelvis (osteotomy) depending on the severity of the condition and the shape of the femoral head.
Slipped Capital Femoral Epiphysis
Slipped capital femoral epiphysis (SCFE) is a common hip disorder in adolescents causing slippage or separation of the femoral head (ball at the upper end of the femur bone) from the weakened epiphyseal growth plate (growing end of the bone).This condition often develops during the rapid growth period after the onset of puberty, and may affect one or both legs at a time. The separation may be caused by an injury or other factors such as obesity and hormonal imbalances. SCFE commonly occurs in children between 11 and 15 years and boys are more likely to develop the condition than girls.
Causes
The exact cause of SCFE remains unclear; however, the presence of certain factors may increase the risk of your child developing this condition. These include:
- Obesity: SCFE is more common in children who are obese and have rapid growth. This may be attributed to excess pressure on the growth plate.
- Endocrine disorders such as diabetes, thyroid disease and growth hormone abnormalities (acromegaly)
- Kidney diseases
- Radiation therapy or chemotherapy for childhood leukemias
- Steroid medications
- Family history of the disorder
Types of SCFE
SCFE is classified into two types, stable and unstable SCFE, based on the severity of pain and damage.
- Stable SCFE (mild slip): The condition is considered mild or stable if the child is having pain or stiffness in the knee or groin area but can manage to walk and may limp. Symptoms worsen with activity and subside with rest. In stable SCFE the child is able to walk with or without the help of crutches.
- Unstable SCFE (severe slip): Any major blow such as a fall or sports injury may cause unstable SCFE. The child may have severe pain and stiffness that may limit movement. The child may not be able to walk or even put weight on the affected side.
Signs and Symptoms
Children with SCFE will exhibit certain characteristic symptoms that may even help the physician in assessing the type of SCFE. The signs and symptoms of stable SCFE include:
- Stiffness in the hip
- Pain in the groin, the thigh or the knee that lasts from several weeks to months
- Limping while walking
- Restricted movements of the hip
- Outward twisting of the leg
The signs and symptoms of unstable SCFE include:
- Severe pain similar to that felt during bone fracture
- Inability to move the affected leg
Diagnosis
Your doctor will diagnose the condition based on a careful medical history and physical examination where the walking pattern and hip movements will be monitored. X-rays of the hip confirm the diagnosis. Other imaging tests that may be ordered include:
- Bone Scanning: Bone scans help in the early detection of children at risk of avascular necrosis and chondrolysis, common complications of SCFE.
- Computed Tomography Scan: Computed Tomography (CT) scans reveal the degree of slippage.
- Ultrasonography: Ultrasound scan helps to distinguish between stable and unstable slip.
- Magnetic Resonance Imaging Scan: Magnetic resonance imaging (MRI) scan may suggest possible complications such as avascular necrosis.
Treatment
The goal of treatment in SCFE is to prevent progression or worsening of the slippage and is accomplished through surgery. Surgery is usually performed within 24-48 hrs of diagnosis.
Surgical Therapy
The surgical procedures available for correcting stable Slipped Capital Femoral Epiphysis include
- Internal fixation (pinning) Bone-graft epiphyseodesis
- Corrective osteotomy
Internal fixation (pinning): This surgery is performed in a hospital setting under general anesthesia. The patient may be positioned on their back during the procedure. The surgeon will make a small incision near the hip. With the use of fluoroscope (X-ray machine that captures continuous real-time /images which are displayed on the TV monitor) as a guide, the surgeon will insert a metal screw or pin through the thighbone and the growth plate so that they are held in place. Your surgeon may use either a single central pin or multiple pins.
- Bone-graft epiphyseodesis: In bone graft epiphyseodesis the surgeon exposes the hip through iliofemoral approach. A rectangular shaped piece of bone is removed from the front part of the femoral neck. A tunnel is created through the growth plate and several corticocancellous strips taken from iliac crest bone are pushed into the tunnel across the femoral physis so that growth plate closure can be achieved.
- Corrective osteotomy: The surgeon exposes the hip by the anterior Smith-Petersen or anterolateral approach. A piece of bone is removed from the metaphysis of the femoral neck. This allows the epiphysis to be repositioned on the metaphysis without affecting epiphyseal blood supply. When the femoral neck gets shortened, the epiphysis is reduced and internally fixed with the help of 3 pins. Although, this procedure is anatomically sound, it is more invasive and may pose serious complications such as avascular necrosis and chondrolysis.
- Surgical correction of unstable slipped capital femoral epiphysis can be done with internal fixation method where your surgeon makes a small incision near the hip and under the guidance of fluoroscope may advance the screw through the metaphysis, growth plate and epiphysis such that the screw holds all three structures in place.
Joint Preserving Surgery of the Hip
The hip joint is one of the body's largest weight-bearing joints and is the point where the thigh bone (femur) and the pelvis (acetabulum) join. It is a ball and socket joint in which the head of the femur is the ball and the pelvic acetabulum forms the socket. The joint surface is covered by a smooth articular cartilage that cushions and enables smooth movements of the joint.
Hip pain has become a common problem particularly in sportspersons having vigorous activities. The main region behind the development of hip pain is due to changes in the shape or structure of the ball and socket type of hip joint.
The treatment options for the management hip disorders such as excruciating hip pain and hip dysfunction, in young patients, have been limited. However, the newer minimally invasive techniques have been found to be beneficial in these patients and these also avoid the need of hip replacement. Some of the common hip preservation surgical procedures include peri-acetabular osteotomy, proximal femoral osteotomy, open hip debridement, hip arthroscopy and cartilage restoration procedures.
Hip arthroscopy is an excellent surgery that has helped many patients restore their hip function and alleviate pain originating from their hip. Hip arthroscopy, is a minimally invasive surgery that is performed through very small incisions to evaluate and treat a variety of painful hip conditions. An arthroscope is a pencil-sized instrument that has a small lens and lighting system at its one end. The arthroscope magnifies and illuminates the structures inside the body with the light that is transmitted through fiber optics. It is attached to a television camera and the internal structures are seen on the television monitor.
A variety of painful conditions can be treated using this technique. Many of his patients are able to return to activities that they were unable to do for years because of pain and limited range of motion.
Hip arthroscopy may be indicated in following conditions:
- Debridement of loose bodies: Bone chips or torn cartilage debris cause hip pain and decreased range of motion and can be removed with hip arthroscopy.
- Repair of torn labrum: The labrum lines the outer edge of the “socket” or acetabulum to ensure a good fit. Tears can occur in the labrum causing hip pain.
- Removal of bone spurs: Extra bone growth caused by injury or arthritis that damages the ends of the bones cause pain and limited joint mobility.
- Restoration and reconstruction of joint surfaces: Injury to the articular cartilage can lead to arthritis. If treated early by arthroscopy the development of arthritis may be delayed or even prevented altogether.
- Evaluation and diagnosis: Patients with unexplained pain, swelling, stiffness and instability in the hip who had no success with non-operative treatments may undergo hip arthroscopy for evaluation and diagnosis of their condition.
Hip preservations surgeries are also indicated in patients with cartilage defects, to preserve the hip and to restore its functionality.
The articular surfaces of the hip joint are lined by a cartilage, known as articular cartilage. It has a smooth surface which allows the articular surfaces to slide over one another with minimal friction. Articular cartilage is often damaged by injury or normal wear and tear. Articular cartilage, when damaged or worn away, the affected joint becomes painful, stiff, and has limited range of motion. As the articular cartilage has limited ability to heal by itself, surgical repair may be required to stimulate the growth of new cartilage. Articular cartilage restoration relieves pain, improve function and can delay or prevent the onset of arthritis in the joint.
Cartilage restoration can be achieved using different techniques.
- Microfracture surgery: Microfracture surgery is appropriate for patients having single lesion and healthy subchondral bone. Microfracture can be done using an arthroscope a long, thin device with a tiny camera attached at the end to see inside your knee. Your surgeon uses a small pointed tool called an awl to make very small holes, microfractures, in the bone underlying the cartilage called subchondral bone. This stimulates the healing process by increasing the blood flow to the surface which brings in new cells that build new cartilage.
- Drilling: This technique involves use of a surgical drill or a fine wire to make multiple small holes through the damaged area to penetrate the subchondral bone. This generates a healing response within the defect. As the heat produced during drilling can cause injury to some of the tissues, it is considered less accurate than microfracture.
- Abrasion arthroplasty: Abrasion arthroplasty can be done using an arthroscope. This technique is similar to drilling, rather than drills or wires, high speed burrs are used to remove the damaged cartilage and to penetrate the subchondral bone.
- Autologous chondrocyte implantation: Autologous chondrocyte implantation (ACI) is a two-step procedure; first step is an arthroscopic surgery to remove the tissue containing healthy cartilage cells from an area of the bone that does not carry weight. These cells are cultured and multiplied in laboratory over a 3- to 5- week period. In second step, the newly grown cells are implanted through an open surgical procedure, or arthrotomy. During this surgery a periosteum, layer of bone-lining tissue is sewn over the area of damaged cartilage. Once the area is sealed with fibrin glue the cultured cartilage cells are injected underneath the periosteal cover.
This procedure is appropriate for patients with single lesion of large area. As the patient's own cells are used chances of rejection is not a concern. However it is a two-step procedure, requiring large incision and lengthy recovery.
- Osteochondral autograft transplantation: In this procedure healthy cartilage (graft) taken from a non-weight-bearing areas is transferred to a damaged area of the knee. The graft is taken as a cylindrical plug of cartilage and underlying bone. Then the graft is matched with damaged area and transplanted into place. This leaves a smooth cartilage surface in the joint. Transplantation may be performed using a single plug or by mosaicplasty where multiple plugs are used.
This technique is used for patients with small areas of cartilage damage because of the limited availability of the healthy cartilage from the same joint.
- Osteochondral allograft transplantation: During this technique tissue graft taken from a cadaver donor, known as allograft is used to repair the damaged cartilage. Allograft may be used if the cartilage defect is too large for an autograft.
Rehabilitation
Your surgeon may recommend physical therapy following any of the hip preservation surgeries to strengthen the joint and the muscles and help restore mobility to the hip joint.
Labral Tears and Other Cartilaginous/Soft Tissue Conditions About The Hip
Labrum is a ring of strong fibrocartilaginous tissue lining around the socket of the hip joint. Labrum serves many functions where it acts as shock absorber, lubricates the joint, and distributes the pressure equally. It holds the head of the femur in place and prevents the lateral and vertical movement of the femur head with in the joint. It also deepens the acetabular cavity and offers stability against femoral head translation.
Labral tear may be caused by trauma, femoroacetabular impingement (FAI), hip hypermobility, dysplasia, and degeneration. It is one of the rare conditions and is common in athletes playing sports such as ice hockey, soccer, golf and ballet. Structural abnormalities may also cause hip labral tear. Patients may have hip pain, clicking and locking of joint and restricted range of motion. Patients may also experience dull pain on movement of hip joint that may not subside on rest. Hip labral tear is often diagnosed with symptoms, history, physical examination and radiological techniques. Magnetic resonance arthroscopy may be more appropriate for diagnosing hip labral tear.
Your doctor may start with conservative treatment prescribing nonsteroidal anti-inflammatory drugs and advising you to rest. These methods may offer symptomatic relief while surgery is required to repair the torn labrum. Your doctor may perform arthroscopic surgery using fiber-optic camera and surgical instruments through the smaller incisions. Depending on the severity of tear, the damaged or torn labrum may be removed or may be sutured.
Hip Dysplasia/Subluxation/Dislocation of the Hip in Cerebral Palsy
Hip dysplasia is a condition which is seen in infants and young children as a result of developmental problems in the hip joint. The femur (thigh bone) partially or completely slips out of the hip socket causing dislocation at the hip joint. It is most common in first born baby with family history of the disorder. The exact cause for hip dysplasia is not known. Genetic factors play an important role in causing this birth defect.
The common symptoms of hip dysplasia include:
- Position of the legs may differ (dislocated hip may cause leg on that side to turn outwards)
- Restricted movement on the side of hip dislocation
- The leg may appear shorter on the side where hip is dislocated
- Skin folds of fat on the thigh or buttocks may appear uneven
In normal hip, the head of the femur (thigh bone) fits well into the socket (acetabulum) whereas in hip dysplasia, the socket and femoral head are not congruent because of their abnormal development. Patients with hip dysplasia may have undergone one or more hip operations during their childhood which might have caused considerable skeletal changes and scarring of the soft tissues. Secondary osteoarthritis may develop later in life which may cause pain and stiffness in the hip. This is an indication for total hip replacement surgery. During this surgery, your surgeon enlarges and prepares the socket to receive the acetabular component. A bone graft may sometimes be placed to recreate the roof of defective hip socket.
Femoro-Acetabular Impingement
Femoroacetabular impingement (FAI) is a condition where there is too much friction in the hip joint from bony irregularities causing pain and decreased range of hip motion. The femoral head and acetabulum rub against each other creating damage and pain to the hip joint. The damage can occur to the articular cartilage (the smooth white surface of the ball or socket) or the labral tissue (the lining of the edge of the socket) during normal movement of the hip. The articular cartilage or labral tissue can fray or tear after repeated friction. Over time, more cartilage and labrum is lost until eventually the femur bone and acetabulum bone impact on one other. Bone on bone friction is commonly referred to as Osteoarthritis.
FAI impingement generally occurs as two forms: Cam and Pincer.
CAM Impingement: The Cam form of impingement is when the femoral head and neck are not perfectly round, most commonly due to excess bone that has formed. This lack of roundness and excess bone causes abnormal contact between the surfaces.
PINCER Impingement: The Pincer form of impingement is when the socket or acetabulum rim has overgrown and is too deep. It covers too much of the femoral head resulting in the labral cartilage being pinched. The Pincer form of impingement may also be caused when the hip socket is abnormally angled backwards causing abnormal impact between the femoral head and the rim of the acetabulum.
Most diagnoses of FAI include a combination of the Cam and Pincer forms.
Symptoms of FAI
Symptoms of femoroacetabular impingement can include the following:
- Groin pain associated with hip activity
- Complaints of pain in the front, side or back of the hip
- Pain may be described as a dull ache or sharp pain
- Patients may complain of a locking, clicking, or catching sensation in the hip
- Pain often occurs to the inner hip or groin area after prolonged sitting or walking
- Difficulty walking uphill
- Restricted hip movement
- Low back pain
- Pain in the buttocks or outer thigh area
Risk Factors
A risk factor is something that is likely to increase a person’s chance of developing a disease or condition. Risk factors for developing femoroacetabular impingement may include the following:
- Athletes such as football players, weight lifters, and hockey players
- Heavy labourers
- Repetitive hip flexion
- Congenital hip dislocation
- Anatomical abnormalities of the femoral head or angle of the hip
- Legg-Calves-Perthes disease: a form of arthritis in children where blood supply to bone is impaired causing bone breakdown.
- Trauma to the hip
- Inflammatory arthritis
Diagnosis
Hip conditions should be evaluated by an Orthopaedic hip surgeon for proper diagnosis and treatment.
- Medical History
- Physical Examination
- Diagnostic studies including X-rays, MRI scans and CT Scan
Treatment Options
Conservative treatment options refer to management of the problem without surgery. Nonsurgical management of FAI will probably not change the underlying abnormal biomechanics of the hip causing the FAI but may offer pain relief and improved mobility.
Conservative treatment measures
- Rest
- Activity Modification and Limitations
- Anti-inflammatory Medications
- Physical Therapy
- Injection of steroid and analgesic into the hip joint
Surgical treatment
Hip arthroscopy to repair femoroacetabular impingement is indicated when conservative treatment measures fail to provide relief to the patient.
Proximal Femoral Focal Deficiency
Coming soon
Femoral Deformity/Fractures in Osteogenesis Imperfecta
Coming soon